Risk Stratification, Coronary Syndromes, Pathophysiology
Risk Stratification is a process of identifying the likelihood of disease and the possibility of having a future cardiac event. These cardiac events are classified as either soft or hard:
Soft events : Percutaneous coronary intervention (PCI) ; Coronary artery bypass grafting (CABG)
Hard events: Myocardial infarction; Cardiac death
Risk stratification provides critical information to the physician for determining what course of action should be taken both diagnostically and therapeutically. Risk stratification of patients with chronic stable angina is the next concern that the physician must face. The goal is to manage the patient based on the results of the clinical assessment and risk analysis. Obviously the objective is to determine the proper course of treatment and prevent further progression of disease and adverse outcomes, e.g., nonfatal myocardial infarction (MI) or cardiac death (hard events). ACC/AHA/ACP-ASIM guidelines describe a patient’s risk as a function of the following factors:
- Left ventricular function—this is the strongest predictor of survival from CAD
- Extent and severity of atherosclerosis
- History or evidence of coronary plaque rupture signifying an increased risk of a hard event
- Extent and severity of provocative ischemia
- General health and/or the presence of other noncardiac, comorbid conditions
Coronary Syndromes
In the evaluation of coronary artery disease, there are a wide spectrum of symptoms and signs that have been categorized according to the severity of the disease. The acute coronary syndromes range from patients who are asymptomatic to those experiencing congestive heart failure and, finally, death.
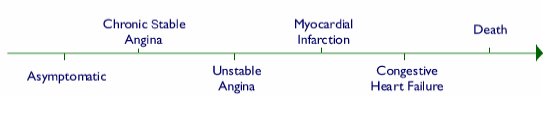
Stable angina is the first coronary syndrome associated with chest pain, usually associated with exertion or emotional stress.
Statistics report that there are over 6 million people in the United States with angina. With managed care and the state of the healthcare environment in the United States, it is imperative that the proper clinical assessment, risk stratification and treatment options be considered for quality of care and cost-effectiveness.
The physical examination and history obtained by the physician helps determine the diagnostic course of action.
After a complete history (with risk factor analysis) and physical examination, the patient is assigned a low, intermediate, or high probability of CAD. In the asymptomatic patient, the history is critical for identifying family history and/ or other risk factors.
|
|
 |
|
|
Asymptomatic Patient
|
Chronic Stable Angina
|
The next stage along the continuum of coronary syndromes is unstable angina, also referred to as coronary insufficiency and/ or preinfarction angina. A patient with unstable angina experiences pain at lower workloads or even at rest.
Symptoms may occur at greater frequency, greater severity, and longer duration than stable angina. These progressive symptoms are the result of significant flow limitation within a coronary artery. Patients with unstable angina are at a higher risk of a hard event-myocardial infarction and cardiac death.
An electrocardiogram indicating an ischemic pattern can facilitate the diagnosis of CAD. The Agency for Health Care Policy and Research (AHCPR) outlines some characteristic patterns of various stages of CAD in the clinical practice guidelines for unstable angina. Once the likelihood of disease is established, risk stratification must be considered
to determine short-term risk of a future event and assessing the patient’s probability of survival.
The primary goal of risk stratification in the unstable angina patient is to improve coronary flow and reduce the likelihood of any hard events. AHCPR recommends that low-risk patients undergo risk factor modification and medical therapy, whereas high-risk patients proceed directly to angiography; intermediate-risk patients proceed to noninvasive testing. The role of noninvasive testing, specifically radionuclide imaging, will be described as it relates to defect size on myocardial perfusion imaging.
Clinical management of this patient would include medical therapy
(aspirin, beta blockers, antianginal drugs, and heparin) and risk factor modification. However, depending on the patient’s clinical impression, further noninvasive testing (nuclear imaging) and/ or invasive intervention (catheterization) may be necessary.
Moving along the path of coronary syndromes, the possibility of a hard event becomes very real, ultimately resulting in death. Myocardial infarction (MI) occurs when there has been a total occlusion of a coronary artery. This results in cellular jeopardy of the myocardium and potential death of the patient.
The possibility of death occurring within the first 24 hours after MI is a major concern. Upon presentation, the physician must obtain an ECG. If the ST-segment is elevated, thrombolytic therapy should be initiated immediately. If the ST-segment is not elevated, further clinical assessment (including cardiac enzymes) should focus on risk stratification. Risk assessment usually is not considered until the second or third day post-MI.
The goal of risk stratification in post-MI patients is to identify the level of risk and the risk of future cardiac events. The objectives for diagnosis and treatment are to:
• Identify the extent and severity of disease
• Salvage jeopardized myocardium
• Restore and improve coronary flow
• Prevent mortality
First, the patient’s symptoms should be stabilized and the risk level should be identified. According to the clinical guidelines for Risk Stratification After Myocardial Infarction, during an uncomplicated MI the high-risk patient will probably proceed directly to cardiac catheterization to identify the extent and severity of disease and to initiate revascularization. The low- and intermediate-risk patient may undergo noninvasive testing (radionuclide imaging) to evaluate myocardial function and viable myocardium. A critical factor for risk assessment in the post-MI patient is identifying the left ventricular ejection fraction (LVEF). An LVEF < 40% dictates aggressive management while an LVEF > 40% usually allows conservative management including noninvasive testing.
Physicians can encounter serious difficulties managing patients who experience a complicated MI. These patients may have a host of other problems such as congestive heart failure, ventricular dysfunction, mechanical dysfunction, various rhythm disturbances, or cardiomyopathy. The physician must aggressively treat these disorders on a patient-by-patient basis.
Congestive Heart Failure
Congestive heart failure (CHF) is classified as one of the coronary syndromes. However, CHF may not be a definite progression along this continuum because most patients who experience an MI do not necessarily progress to CHF. The symptoms of CHF include shortness of breath, orthopnea, and peripheral edema. CHF is also a manifestation of impaired left ventricular function and marked left ventricular dilatation after a significant MI. This presents a dilemma because CHF may be characterized as both a soft event (based on symptoms) and a hard event (based on a low ejection fraction).
Upon presentation, a clinical assessment is performed with the appropriate diagnostic procedures to confirm CHF. The primary goal in the treatment of CHF is to improve daily functioning, attempt to restore ventricular function, and prolong survival. Patient management consists of medical therapy,
including aspirin, ACE inhibitors, digoxin, nitrates, diuretics, beta blockers, and oxygen therapy. Risk factor modification, especially smoking cessation, is also needed for patient management.
Managing patients with CHF is very difficult because the severity of the disease differs in each patient. However, revascularization in CHF
patients may improve global and regional function and improve the symptoms.
Cardiac Death is the end stage of the coronary syndromes. Other causes of cardiac death include:
- Complete obstruction of a major coronary artery, causing global cardiac dysfunction
- Cardiac rupture
- Persistent arrhythmias despite treatment.
Radionuclide Imaging in Acute Coronary Syndromes
Acute chest pain brings over 6 million patients annually to emergency departments in the Unites States. Because the majority of these patients have normal or nondiagnostic ECG findings, rule out for MI, and less than half of these patients are found to have a cardiac etiology for their pain, medical centers have established dedicated chest pain units to safely and accurately evaluate these patients with chest pain protocols. Most chest pain protocols first exclude myocardial infarction with serial serum markers of myocardial injury (troponin), resting echocardiography, or resting SPECT MPI.
Stress (and Rest) Myocardial Perfusion Imaging may be performed with exercise or pharmacologic vasodilation to facilitate the complete evaluation of chest pain patients prior to discharge from the Emergency Department. It is possible to cut the number of hospital admissions in half with such protocols, allowing for safe discharge of ED patients at or near 24 hours from time of arrival.
Summing Up Coronary Syndromes
We have discussed the various disease states comprising the coronary syndromes,
practice guidelines and treatment algorithms for each of these syndromes. All diagnostic and therapeutic procedures covered in the next
section play an integral part in the risk assessment and stratification of patients who have coronary heart disease.
Risk stratification assists the physician in identifying the likelihood of disease, the extent and severity of disease, the probability of future events, and survival.
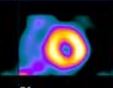
It is now evident that noninvasive testing, particularly nuclear cardiology, plays an integral part in the assessment and management of patients who are diagnosed with coronary artery disease. The quality images generated through the use of state-of-the-art equipment and sophisticated radiopharmaceuticals are critical to the value that nuclear cardiology provides to a physician. Nuclear medicine technologists are the key players in this quality.
Pathophysiology: Consequences of Disease
When myocardial oxygen demands increase, they are normally met by an increase in myocardial blood flow. In the LV, flows in resting individuals are about 80 to 100 ml/ min/ 100g and, with increased demands, normally can increase 3-5 fold. Flow in ventricular walls may be inhomogeneous, and tends to be less in the outermost third (subepicardium) than in the innermost third (subendocardium).
The deep layers of the heart are more susceptible to ischemia when the supply/ demand balance changes. Ischemic tissue contracts less effectively or not in unison with the remaining normal ventricle. This asynergy underlies the development of congestive failure in many patients with coronary heart disease.
Coronary Insufficiency: the demand for energy exceeds supply. Coronary Insufficiency may be localized in the case of coronary atherosclerosis, or generalized with aortic valvular disease or cardiac hypertrophy. In coronary artery disease, stress evokes a greater than normal increase in coronary flow probably because of inefficient contraction.
Impaired cardiac filling
There may be impaired cardiac filling in chronic constrictive pericarditis, which leads to thickening and sometimes calcification of the layers of the pericardium. Stenosis of the mitral and tricuspid valve, clots, or tumors may also depress cardiac filling.
Intrinsic myocardial pathology
Many infiltrative, inflammatory, or tumor stages may influence myocardial contractility causing failure of the myocardial pump.
A group of diseases known as myocardiopathies in which there is destruction of the functional myocardial cells are classified as hypertrophic, dilated and restrictive. Cardiac dilatation and myocardial hypertrophy are forms of compensatory reserve, long-term effects of which usually lead to cardiac failure.
- 5a: CV Disease
- 5b: Coronary Syndromes
- 5c: Atherosclerosis
- 5d: Myocardial Infarction
- 5e: Stress Testing
- 5f: Cardiac Medications
- 5g: Revascularization
- Lesson 5 REVIEW