Cardiovascular Disease: Assessing the Patient
Cardiovascular disease includes: High blood pressure, Coronary artery disease, Stroke, Congestive heart failure, and Congenital cardiovascular disorders. CVD is the number-one cause of death in Americans, killing twice as many people as cancer.
Within the past two decades, many new methods have been developed for diagnosis and management of CVD.
A vast national and private effort has worked diligently to:
- Improve the process of identification of CAD
- Educate patients on risk factors and other contributing causes of heart disease
- Stress the importance and possibility of prevention, risk factor modification, and rehabilitation
History and Physical, Laboratory Evaluation
Total patient management is a process which includes assessing the patient’s status, obtaining the proper diagnostic procedures, making an accurate diagnosis, and providing treatment to relieve symptoms and restore health. A patient who presents to the emergency department with chest pain does not always have heart disease. Some noncardiac causes of chest pain include pulmonary embolism, gastrointestinal problems, and pneumonia. The physician must interview and examine the patient before beginning any tests or treatment.
To assess a patient for clues that will lead to a diagnosis, the physician first takes a thorough history, in which the patient also describes the symptoms that he or she is experiencing. Next, the physician performs a physical examination. Thus, the physician can determine the patient’s natural history and evaluate the symptoms. For example, a patient with chest pain who is later determined to have had a myocardial infarction will likely present with different signs and symptoms from a patient who is later determined to have had a pulmonary embolism.
Based on the patient’s initial assessment, the physician next orders certain diagnostic tests. The first level of exams usually involves laboratory procedures, including blood work. Depending on those results, the physician may order a special anatomic and physiologic examination, which includes more sophisticated tests such as x-rays and ECGs.
Getting a working diagnosis involves careful assessment to identify clues,
while matching the clues to a disease process. This preliminary, or working,
diagnosis may necessitate further assessment and management of the patient
by specialists. Once the physician makes a diagnosis, the patient follows a
specific treatment plan designed to meet his or her needs.
Laboratory tests provide information on the cardiopulmonary status, the presence of concomitant disease or complications of myocardial infarction (MI), and the patient’s response to therapy. The following descriptions pertain only to those biochemical markers that provide diagnostic information on patients with suspected heart disease. Once a diagnosis is made and the patient is placed in the appropriate critical care area, other routine blood tests are performed to monitor the patient’s status.
Pretest Likelihood of Disease
Calculation of the patient’s pre-test likelihood of coronary artery disease is the first goal of triage, based on Bayes Theorem. Likelihood of disease is derived on the basis of clinical presentation, risk factors, and symptoms. This determination is based on the presence of chest pain, the patient’s age and gender, and the existence of other risk factors. Consider the following three types of chest pain:
- Typical angina. The classical pattern of substernal discomfort precipitated by stress, emotion, or exertion and relieved by rest or nitroglycerin.
- Atypical chest pain. Characterized by the presence of two of the patterns associated with typical angina.
- Non-anginal chest pain. Characterized by the presence of none of the patterns associated with typical angina.
Sensitivity = [ (True Positive) divided by (True Positive + False Negative) ] X 100
Specificity = [ (True Negative) divided by (True Negative + False Positive) ] X 100
Positive Predictive Value = [ (True Positive) divided by (True Negative + False Positive) ] X 100
Negative Predictive Value = [ (True Negative) divided by ( True Negative + False Positive ) ] X 100
Bayes’ Theorem
The application of Bayes’ Theorem is critical since sensitivity and specificity will better define the presence or absence of disease. Although not all physicians utilize this approach, it has been shown to be a more cost-effective use of diagnostic testing, especially in a managed care environment.
- Sensitivity: The frequency of a true positive test result in a population with disease.
- Specificity: The frequency of a true negative test result in a population without disease.
- False Negative: The frequency of a negative test result in a population with disease.
- False Positive: The frequency of a positive test result in a population without disease.
Once the physician has identified the patient’s risk for CAD, he/ she must establish the extent and severity of disease. Extent is evaluated by the number of diseased vessels: single-vessel or multi-vessel. Severity is based on the degree of coronary stenosis.
Complementary Diagnostic Imaging Modalities
Because of the prevalence of CVD, physicians depend on diagnostic modalities to direct their medical decisions.
Modalities that complement Nuclear Cardiology in the diagnosis of coronary artery disease include Echocardiography, Cardiac CT, Cardiac MRI, and Cardiac Catheterization.
The emphasis in today’s managed care environment is not only on diagnosis, but also on improved prognostication and patient management. Nuclear cardiology procedures are important in risk stratification and identification of a treatment plan. Risk stratification is the process of identifying patients who are at low, mild-to-moderate, or high likelihood of disease and assessing the risk of a future cardiac event.
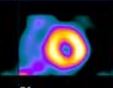
Nuclear cardiology is the only noninvasive procedure that can assess myocardial perfusion and function simultaneously. This advance has been made possible by the development of technetium-99m-based cardiac imaging agents. Nuclear imaging is used more and more to assess the extent and severity of disease in a patient with known or suspected coronary artery disease.
- 5a: CV Disease
- 5b: Coronary Syndromes
- 5c: Atherosclerosis
- 5d: Myocardial Infarction
- 5e: Stress Testing
- 5f: Cardiac Medications
- 5g: Revascularization
- Lesson 5 REVIEW